
Shin Pain or Shin Splints – Cause and Correction
A frequent complaint in runners is shin pain or shin splints, with the most common condition known as Medial Tibial Stress Syndrome (MTSS) making up 16% of all running injuries. It certainly isn’t comfortable, with pain on the inside of leg, often bilateral, and tender on the touch covering an area greater than 5cm.
Plyometric type activities like running and jumping are usually the aggravating factors. Pain can sometimes appear initially at a workout, disappear as warming up and return on post-exercise. It is a condition that can increase in severity with pain remaining during exercise and continuing for days.
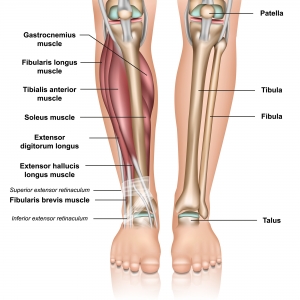
It is often thought that one of the main causes is due to the soleus muscle pulling on the tibial bone, causing periosteal (the membrane that covers the outer surface of the bone) irritation as well as underlying bone irritation from increase loading.
Other Causes of Pain and Locations
There are numerous causes of lower leg pain and it is important to differentiate between them. A very focal pain could potentially be a stress fracture. Stress fractures often tend to be worse with activity and won’t warm up like the early stages of MTSS.
Pain directly at the front of the leg (anterior) could be anterior compartment syndrome or a tibial stress fracture.
Posterior calf pain or pain at the back of the calf area, a condition called Deep Posterior Compartment Syndrome is to be considered. This often presents as more cramping /burning type pain and is likely to send pain and/or pins and needles into the foot.
MTSS is quite localised, so if there is any altered sensations or pain in the foot area, then it could be posterior compartment syndrome, nerve issues more proximal, for example from the lumbar (low back) spine, distal neuropathies for example diabetes, or vascular involvement in the leg. A simple ruling out for functional foot problem is also important as there are many bones in the feet. Flat feet or very high arches can cause a mechanical issue within the movement patterns of the foot during any gait activity and can also lead to pain and/or discomfort in the feet, not always bilaterally.
Just to add to diagnostic confusion, in a study in 2017, 32% of those with MTSS had co-existing pathologies (e.g. anterior tibial stress reaction or muscle pain, calf pain).
Management
Multifactorial causes must be acknowledged for all running injuries including structural, genetic, running mechanics, training loads and tissue qualities including strength and mobility.
Modifying the training load so as not to exceed 4-5/10 regarding pain markers is required. Above this pain score, then cross-training type exercises should be considered.
The biggest strain on the tibial bone is muscle contraction which is greater in running uphill so best avoided in MTSS. Step rate (cadence) increase as well as step width increase are wise to employ as well as trying to reduce impact loading. Visualise running on hot coals (running quietly) instead of stomping like an elephant!
Calf muscle strength is a very important consideration as studies have found that those with MTSS had weaker calves following a single leg raise to fatigue test.
Corrective Procedures
Calf strengthening procedures are best with single leg weighted calf raises adding weights incrementally to keep repetitions under 12. Calf strengthening is important for MTSS to assist in greater absorption of impactful forces as well as strengthening to improve tibial bone strength.
Plyometric exercises (jumping, hopping, skipping) are another great way to improve calf and tibial bone strength. It is important that the strength of the of other leg muscles and hips and pelvis be assessed for any weaknesses and corrected.
Manual therapy could be useful such as Chiropractic Adjustments to the foot bones, tibia, fibula, femur and pelvis bones to address any biomechanical joint dysfunctions and massage and trigger point therapy or dry needling to overly contracted muscles.
Assessing and correcting dysfunctions in the whole kinetic chain is important to remove any contributing factors.
In some cases, foot orthotics might be required, also a change in footwear could be the answer. A compression sleeve or sock can benefit some people.
The duration of MTSS can be quite long with some studies suggesting it can take up to 3 months to run at a moderate intensity with minimal pain, however, it is our experience that if detected early with the application of early treatment protocols, this time can be shortened.
For a free biomechanical foot scan, please contact our Sydney chiropractic clinic for an appointment. It can be the first step to correction!



